Study supporting DUTCH testing – Improved Serum Correlation
Mark Newman, MS
Study supporting DUTCH testing – Improved Serum Correlation
by Mark Newman, MS
I’ve been anxiously waiting for all our data to roll in from an exciting study, and we’re now ready to share it. What we did shows a very distinct advantage to our model of testing with respect to estrogen testing.
{kind=link}

Here is what we did in our study:
- Collected serum, saliva and dried urine samples from a group of women throughout their entire cycle (we included one first-trimester pregnancy case as well)
- Collected serum, saliva and dried urine samples from a group of postmenopausal women (with no history of HRT)
- Serum samples were tested for estradiol (E2) and progesterone (Pg) by the Reproductive Endocrinology Dept at U. of Southern California (USC)
- Saliva samples were mixed, split and sent to 7 different saliva labs (one lab’s data showed no cycle of E2 or Pg in contrast to all other data, so their data was excluded)
- Dried urine samples were tested at our facility by GC-MS/MS for estrogen and progesterone metabolites
- Urine was also tested for LH for premenopausal women to more accurately identify the ovulatory surge of LH and E2
Data Examination
{kind=link}
- Correlation data was examined for saliva and urine relative to serum data
- Data was separated into four groups for E2 (postmenopausal, follicular, luteal, ovulatory) and the pregnancy case was included with ovulatory for E2 and luteal for Pg
- Luteal samples were identified by moving beyond the ovulatory peak and data used if there was a significant increase in serum progesterone (this makes the deck stacked a bit on the side of serum testing, but it makes for a good comparison between urine and saliva)
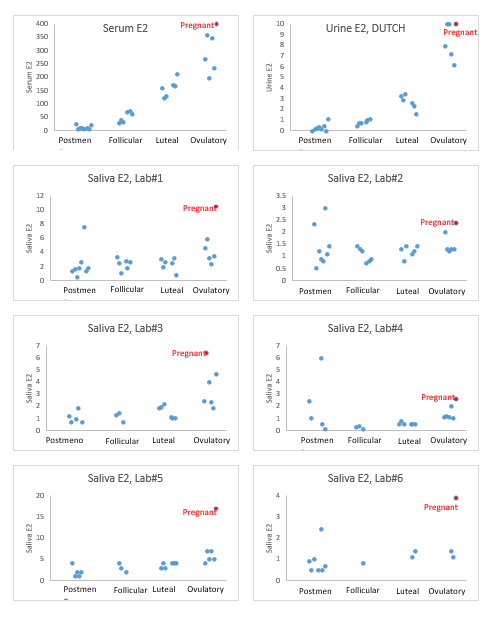
RESULTS!
- R2 values for correlation between serum and urine were improved when compared to the 6 salivary data sets. DUTCH urine data was modestly improved relative to salivary data for Pg and much improved for estradiol.
- While serum and urine testing showed a significant (~10X) difference between premenopausal luteal levels and postmenopausal levels of E2, salivary testing struggled to separate the two groups. Some salivary assays also struggled to separate postmenopausal levels from ovulatory levels.
There are a number of DUTCH testing advantages. My top three are:
- Combining the free cortisol pattern with the metabolites of cortisol
- More accurate testing of estradiol (compared to salivary assays)
- The addition of estrogen metabolites (2-OH, 4-OH, 16-OH, Methylated estrogens etc.)
The above data supports claim #2 above fairly dramatically.
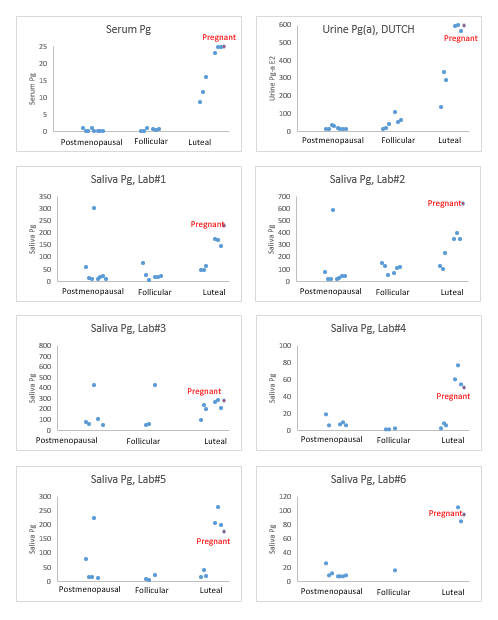
One advantage of urine testing (of estrogens) is that there is about 1000 times more estradiol in urine compared to salivary testing. The concept of testing free estradiol in saliva makes a lot of sense. Practically speaking, it is very difficult to make a test that easily measures the levels accurately and reproducibly. Below you can also see the progesterone data from this study. Progesterone values are a lot easier to measure well in saliva and the data is improved in saliva. Correlation with serum was slightly better with our urine testing compared to the best saliva data. The most basic distinction we are looking for in this data is a clear separation between luteal levels (should be higher) and the other two groups.
Progesterone Data
{kind=link}
- Salivary data was more consistent with serum data for progesterone (except for a couple labs)
- Correlation data compared to serum was best for DUTCH testing but was only slightly worse for the better looking salivary data for premenopausal data
- Salivary data seems to have more potential for showing falsely high results for women who clearly have low progesterone (postmenopausal, no HRT)
Conclusions:
The DUTCH model provides excellent results for reproductive hormones and may be a significant improvement compared to salivary testing. The better saliva assays are a good way to see the timing of hormones (when did I ovulate? Did I have a significant progesterone surge?). DUTCH is a little better for this line of questioning (with our DUTCH Cycle Mapping test) and quite a lot better at determining whether the patient is low, normal or high for their estradiol status. One of the things I have loved about DUTCH testing is how well we can define the patient with respect to estrogen (accurate values AND metabolites) and cortisol (free pattern AND metabolites). This recent study affirmed this, and we hope you will find the same as you use and explore DUTCH testing including DUTCH Cycle Mapping.
Cheers!
TAGS
Laboratory Testing: In-Depth Look at DUTCH Urine Testing
Estrogen and Progesterone
Premenopausal Women
Postmenopausal Women
Functional Laboratory Testing: General
Women's Health